HOME TREATMENT PLAN
Introduction
Thank you for placing your trust in my self-treatment plan that reduces load on the plantar fascia and in turn, reduces the traction of this ligament type structure on the heel, allowing it to repair.
Some of the causes of Plantar Fasciitis also cause problems around the back the heel and Achilles tendon too. I have included information and treatment for the common conditions ( Achilles Tendonitis / Bursitis) in this part of the foot too.
Disclaimer: Please note that DR Karl Lockett is not liable for your foot and ankle condition without consultation and informed consent.
This short course provides the foundations of all treatment plans provided by Dr Karl to his patients in clinic. Some of his local patient’s choose to include other treatments such as shock wave therapy to accelerate the healing but these other treatments are much less likely to work as stand-alone treatments, without the foundations and crucial information provided here.
Patient’s who are compliant and follow all my requests and advice collectively and consistently usually recover quicker than those who only follow some of the treatment advice or who are inconsistent with the approach.
Please do not cherry pick parts of the plan in the hope that you will get a result as my patient results have shown that the treatment of Plantar Fasciitis is multi-factorial.
Hi, I’m Dr Karl, a sports podiatrist with over 20 years clinical experience. I’m the principal practitioner here at Sydney Heel Pain Clinics and the podiatrist to the Sydney Opera House.
As someone who helps people with foot pain, my role is incredibly important because foot pain can significantly impact a person’s quality of life. The heel and arch are common areas of discomfort and pain for many people, and two of the most common causes of heel pain are plantar fasciitis and Achilles Tendonitis.
As someone who has worked with individuals suffering from a range of foot pain conditions for over 20 years, I have gained extensive knowledge and invaluable experience in the world of foot health.
With this experience comes a deep understanding of what works and what doesn’t work when it comes to treating foot pain. I have tried and tested almost every single treatment available for each condition, from traditional methods like rest, ice, massage, spikey balls, night splints, moon boots, acupuncture, compression socks, footwear brands and physical therapy to more advanced treatments like shockwave therapy, cortisone injections, moon boots and arch supports / orthotics.
My extensive experience has allowed me to come to understand which treatments are ineffective and sometimes detrimental in treating certain conditions. This is valuable knowledge, as it allows me to guide my clients away from treatments that may not work for them, saving them time, money, and unnecessary pain.
The Foot and Heel Pain at home treatment plan provided by Dr Karl Lockett has been created using the in house treatment plans that he has used on thousands of patients that he has seen in clinic. The advice provided in this course should be followed carefully and consistently.
By purchasing and using this treatment plan, you acknowledge that Dr. Karl Lockett is not liable for any injuries or damage that may result from your use of the information provided.
For further assistance or if you are unsure what to do before you begin, feel free to contact us via an online form here.
Exclusive Report
From inside the walls of my clinics I bring you this priceless knowledge, formulated from my 20 plus years of experience, in treating Plantar Fasciitis.
- Footwear myths revealed – the 3 worst shoes to buy for Plantar Fasciitis. A surprise leading brand named.
Please note: Cushioning is not your friend and comfortable shoes don’t fix Plantar Fasciitis. Problem shoes are flat / flexible / full off cushioning. Such as-
1: Skechers (the original / traditional style)
2: Nike free – and similar
3: Flip flops / thongs
A small amount of cushioning inside the shoe is ok, but the mid-sole and out-sole must be more rigid and firm. See footwear suggestions below.
- 4 popular types of exercise that keep us happy and healthy but cause debilitating heel pain – stop these now and your pain will stop too!
The following types of exercise place load through the sole of your foot (plantar fascia) and calf muscles:
1: Reformer machine – Pilates.
2: Cycling
3: Downward dogs in Yoga
4: F45 / Cross-fit / Body pump classes – which involve pushing off the front of your foot.
Note: You may cycle if you move your foot forwards on the pedal and push with your heel / arch.
- 3 shocking reasons why your Plantar Fasciitis will not recover soon– unless you act on these findings.
1: Beach walking and bare foot walking stresses and loads the plantar fascia as well as the calf muscles.
2: Your calf muscles are still tight and this pulls through the heel and arch of your foot.
3: You think your foot and ankle is weak and your doing strengthening exercises which loads and irritates the plantar fascia.
- Save your money and stop online shopping for products that claim to cure Plantar Fasciitis – 4 of the most common gimmicks that give nothing more than short term relief.
1: Spikey massage balls
Massage and rubbing the heel can provide short term relief but can irritate the heel and prolong the problem.
2: Vibit and other vibrating devices.
Nothing more than short term pain relief, at best.
3: Heel cushions.
Nothing more than short term pain relief, at best.
4: Night splints / Strasbourg sock
Feedback from patient’s is always the same. They reduce the morning pain slightly, but they are uncomfortable to wear and usually get removed mid-sleep. They don’t help it heal.
- What are the best shoes for Plantar Fasciitis? I reveal what to look for when selecting shoes. I even name some specific brands and models.
1: Slight heel raise – 10-15mm
2: Firm / more rigid mid sole / out sole
3: Closed in – lace ups best but a snug fitting slip-on can be ok.
Brand names revealed in the footwear section of the treatment plan, with video, but in simple terms a firm soled sneaker / sports shoes / tennis shoe /cross trainer is ideal.
- 3 reasons why cortisone injections often fail to treat Plantar Fasciitis permanently.
1: Not done under ultra sound guidance – so the cortisone doesn’t reach the target area.
2: The patient still has very tight calf muscles.
3: The patient continues to wear incorrect shoes.
Other reasons: The patient continues to load the calf / plantar fascia with stretches or exercise.
I often hear patients ask, isn’t cortisone a temporary solution? And this is not necessarily the case. The job of cortisone is to block the inflammatory cycle which in turn reduces pain. After the injection, if the patient continues to nurture the foot in the correct way and reduces the strain / load on the plantar fascia, then it is highly unlikely that the inflammation and pain will return. However, most of the time, when the cortisone does “wear off” and the pain returns, this is usually due to the fact that the patient has not received any other form of treatment or guidance.
- The crucial mistakes that most practitioners make when treating Plantar Fasciitis – Podiatrists and Physios included.
1: They recommend calf raises / strengthening exercises – especially physio’s.
2: They encourage you to stretch the plantar fascia.
3: They suggest cushioned shoes.
- Your muscles need to get LONGER, not STRONGER! The 3 foot exercises that are holding you back Vs my super stretch that will get you walking again.
Most patient’s in my clinic get better when they stop trying to stretch the bottom of the foot. There’s a detailed explanation for this as you work through the treatment plan. But typically, people with Plantar Fasciitis have TIGHT / SHORT calf muscles, NOT weak.
Exercises to avoid:
1: Calf raises
2: Hanging the back of your foot / heel off a step.
3: Pulling your toes back with your hands or by pushing the underside of your toes against a wall.
Intrinsic foot muscles exercises, foot clenches and picking up small objects with your toes can be avoided as they do not help.
Details of the super stretch can be found as you progress through the treatment plan.
Condition Overview
Understanding the distinction between conditions and symptoms is crucial for addressing foot pain effectively. Plantar Fasciitis (PF) and Achilles Tendonitis (AT) are specific diagnoses, while arch pain and outer heel pain are symptoms that may arise from these conditions, among others.
PF and AT are the most frequently encountered diagnoses in our practice. However, other conditions like Peroneal Tendonitis can also lead to outer heel and arch pain, while Tibialis Posterior Tendonitis might cause pain on the inner side of the arch. It’s important to be familiar with these terms, as your practitioner may mention them during consultations, especially if an in-person visit becomes necessary after 8-12 weeks of following an at-home treatment plan.
Not everyone with arch pain has Plantar Fasciitis, and not all PF sufferers experience arch pain; some may have heel pain instead. If you’ve been diagnosed with any of these conditions, it’s essential to concentrate on treating the specific areas where you feel discomfort
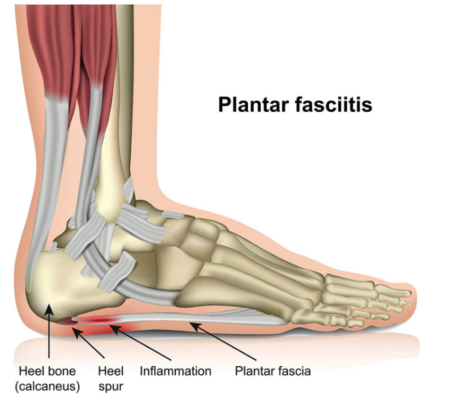
Plantar Fasciitis:
Plantar fasciitis is a painful inflammatory condition that affects the large ligament-type structure at the base of the foot, known as the plantar fascia. This structure connects the base of the heel bone to the toes, supporting the arch and absorbing load when walking.
The plantar fascia can become thickened and inflamed due to irritation at the attachment point, usually caused by repeated tension, stress and strain. The majority of patients experience pain in the heel while some develop pain further forward through the arch of the foot.
“Start-up pain” is almost always a feature and the first few steps of the day are usually uncomfortable. Likewise, Plantar Fasciitis causes pain after being seated and can become increasingly sore as the day progresses.
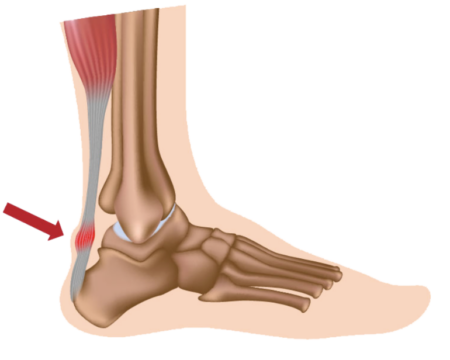
Achilles Tendonitis, Tendinosis or Bursitis (Pain in the back of the heel)
There are two main conditions that affect the Achilles tendon; one is known as Achilles Tendonitis and the other is Insertional Achilles Tendinosis.
Achilles tendonitis is a painful condition that causes dull to sharp pain around the back of the ankle above the heel. It usually involves inflammation around the Achilles tendon or within the sheath that surrounds it. You may most commonly feel pain when pushing off with the foot and can be triggered with activity and exercise. Some patients also experience a creaking or cracking sensation when moving the ankle, this can occur when the damaged or inflamed tendon rubs against the surrounding tissue or tendon.
Insertional Achilles Tendinosis is a condition where the fibres of the Achilles tendon that attach to the heel bone start to break down or degenerate, causing pain at the back of the heel. In some cases, small bony growths called bone spurs can be seen in the same area, but they don’t typically cause pain on their own. Instead, the damage to the tendon around the bone spur can be painful.
Bursitis (Retro calcaneal)
Additionally, there is a small fluid-filled sac called the Bursa located behind the tendon which can also become inflamed and lead to a condition called bursitis. People with bursitis may feel stiffness in the heel area rather than pain.
Arch Pain:
Arch pain can be the result of one or a combination of conditions that develop in the sole of the foot but is most commonly caused by Plantar Fasciitis. The pain in the arch can come on suddenly as in a one off day of increased walking or a sporting event, or progressively over a period of time as in walking in inappropriate shoes. It will often feel worse in bare feet or thongs or flat and flimsy shoes such as ballet flats. Other conditions that cause pain in the arch are Tibialis Posterior Tendonitis and Peroneal Tendonitis.
Outer Heel Pain:
Plantar Fasciitis usually involves the medial (inside area) of the heel but can sometimes affect the lower lateral (outside area) of the heel. In addition to Plantar Fasciitis, another cause of outer heel pain, this time a little higher up and the outer wall of the heel, is Peroneal Tendonitis. Pain, inflammation or irritation to the long tendon coming down the outside of the leg and ankle, inserting into the outer aspect of the foot. Outer heel pain can also be a referred pain from the insertion of the Achilles tendon.
CAUSES FOR ALL CONDITIONS AND PAIN AREAS:
There is no single cause of heel and arch pain. Ultimately, these conditions develop due to an increased load on the plantar fascia / Achilles tendon (or other areas of soft tissue) which causes it to become irritated / inflamed / thickened. Factors such as age, diet, exercise, body weight or environmental conditions such as poor footwear choice can all play a part.
The term ‘pathological’ can be used which means that there is a structural or functional abnormality or damage to the fascia or tendon. Tight calf muscles and soft shoes are a big problem, as are flat feet or high arches and an increase in body weight. Biomechanical issues such as abnormal walking patterns and poor poor foot function can also trigger these conditions.
Patients who suddenly increase the amount or frequency of sporting activity/exercise are also at risk. We saw a big influx of patients with Plantar Fasciitis / Achilles Tendonitis during Covid 19 lockdown as many people suddenly began walking barefoot or in less supportive shoes at home.
One of the most common findings with these conditions is restricted range of motion in the ankle joint due to tight calf muscles. This causes an increase in the amount of tension running through the Achilles tendon which over time will lead to an increase in traction on the heel. The stress on the tendon causes irritation and this leads to inflammation and pain too (Achilles Tendonitis).
CAUSES FOR OUTER HEEL PAIN:
The causes of outer heel pain are outlined above and relate to Plantar Fasciitis and Achilles Tendinosis. If the peroneal tendon is involved this can be affected by lateral ankle sprains and increase in stress due to tight calf muscles.
What To Avoid
The internet is a big place, and misinformation online is widespread. Following online advice can be risky if the person or practitioner who’s making the recommendations does not specialise in these conditions. This can very often lead to patients receiving incorrect information that can prolong the pain and aggravate the condition.
It is important to address the root cause of your condition and prevent the recurrence of the issue.
Here are some common misconceptions (notice how we did not say treatments) seen from patients coming to Sydney Heel Pain clinics;
Plantar Fasciitis
- ‘You need to stretch your plantar fascia’: Yes, stretching your Plantar Fascia can sometimes offer immediate pain relief, temporarily, but this usually prolongs the condition as it increases the strain on the affected tissue.
- ‘You need to strengthen your calves’: Most patients have tight calf muscles, not weak calf muscles so please do not attempt to load and strengthen.
- ‘You need to cushion your heel’: Cushioning feels good temporarily but provides instability. Your foot needs support and stability, not cushioning.
- ‘You need to strengthen your intrinsic foot muscles’: Your foot ligaments provide significant support for your feet, less so the muscles, and Dr Karl has found that foot muscle exercises do not form part of a treatment plan.
Achilles Tendonitis, Tendinosis or Bursitis
- ‘You need to strengthen your calves’: Most patients have tight calf muscles, not weak calf muscles so please do not attempt to load and strengthen.
- ‘You need to load up the tendon to stimulate healing’ – More often than not, this aggravates or prolongs the condition if performed when the pain is present and the condition is acute.
All Conditions:
- ‘You should apply heat’: This usually feels good for a short while but can increase inflammation and pain long term.
Certain stretches and treatments can cause further irritation to the affected area, leading to more severe symptoms and/or longer recovery times. Such as:
Plantar Fasciitis (Including arch pain)
- Rolling your foot on a golf ball
- Rolling your foot on a tennis ball
- Rolling your foot on a frozen water bottle
- Rubbing and massaging the heel
- Heat packs or hot water bottle
- Step stretches
- Stretching the bottom of your foot
- Calf raises
Achilles Tendonitis, Tendinosis or Bursitis
- Calf raises
- Eccentric loading
- Step stretches
- Rubbing and massaging the tendon / back of heel
- Heat packs or hot water bottle
- Soleus stretches (calf stretching with knee flexed)
If you are suffering from any of the conditions; Plantar Fasciitis, Achilles Tendonitis, arch pain or outer heel pain, we recommend reducing/avoiding the following activities.
You should avoid activities that load the forefoot, not the heel directly. When pressure is applied to the forefoot (the ball of your foot or the area just behind the toes), this strains the plantar fascia and loads the calf and Achilles Tendon.
For example:
- Standing or walking on your tiptoes
- Skipping / Jumping
- Lunges
- Downward dogs in yoga
- Pressing on a bar or in stirrups during Pilates
- Cycling while pushing with your forefoot. You should move your foot forward on the pedal and push with your heel or midfoot.
- Steps / Stairs
- Ladders
- Leg press machines at the gym: Keep your heel on the plate
- Quick movement sports such as tennis, basketball or other team sports that involve running and sprinting
- Walking / standing still for extended periods of time such as in Golf
When it comes to taking any medication, you should always consult with your doctor, GP or physician. Dr Karl’s treatment plans do not involve medications.
Anti-Inflammatories: These can sometimes reduce the pain but only temporarily. Usually, the pain will come back when you stop taking the medication. These pharmaceuticals are therefore masking the problem.
Painkillers: The same can be said for painkillers such as paracetamol.
Arch Supports: Generic arch supports are hit and miss. They can help, but they sometimes apply too much pressure against the arch of the foot and can increase the symptoms (or even cause) Plantar Fasciitis. Most people have very subtle differences between their left and right foot but generic shoe inserts are made symmetrically. If you try a pair and they feel like a golf ball in your shoe, or there is too much pressure against the sole of your foot, please remove.
Heel Cushions: While these may provide slight relief, temporarily, they create an unstable base for the heel to sit on and this leads to hypermobility. In other words your heel can wobble inside the shoe leading to further irritation.
Tiger Balms, Voltaren Gel & Deep Heat: These topical ointments may feel nice but are not proven to help these conditions heal. The same can be said for heat packs.
Night splints: Most patient’s report that the morning pain is less if they sleep with a night splint. However, not many people can last through the night and will remove it around 1am! Night splints are not proven to assist the healing process.
Compression socks: Again, they feel nice as they hug the feet but they do not provide enough support to reduce strain on the affected fascia / tendon, in order to help it heal.
Your Treatment Plan
Almost all of Dr Karl’s new patients that present with heel pain have a limited range of ankle joint dorsiflexion due to tight calf muscles. Unfortunately, most calf stretches result in strain through the plantar fascia due to the position of the foot during the stretch.
Dr Karl’s calf stretching technique helps to unload the plantar fascia and Achilles Tendon by releasing the heel during gait.
‘The Super Stretch’ – For all conditions
This calf stretching technique with the foot supinated (rolled out slightly) does not load the plantar fascia. The foot arch is lifted slightly which shortens the foot and removes strain on the connective tissue, which in turn reduces traction on the base of the heel.
This should be the only stretch that you do during your rehabilitation. You must hold each stretch for at least 1 minute and do 3 on each leg, repeating up to 4 times a day until you have good calf range. This may take a few weeks to achieve.
Please note if you naturally have a high arch when standing (not assessed when sitting or lifting your foot off the floor) then you may not need to roll your foot out, but please ensure your foot / ankle does not roll inwards. If you’re still unsure, please watch the video below for an easy to understand demonstration.
How to Release The Heel: (All Conditions)
- Deep tissue massage
- The application of magnesium cream, massaged into the belly of the calf muscles
- Releasing with a foam roller or rolling pin
- The use of a handheld massage gun
- You may also wish to visit a practitioner who offers dry needling with acupuncture needles.
PLEASE DO NOT APPLY TAPE IF YOU HAVE AN ALLERGY TO IT. Although a tape allergy is rare, it can affect some people and cause severe itching and inflammation. Please remove immediately if so, and wash the skin on your feet immediately. If the discomfort persists you may wish to purchase steroid cream from the pharmacy.
Properly strapping the foot can be of immense importance in supporting some foot conditions and aiding in the healing process.
If you’re struggling with an Achilles tendon condition, strapping techniques do not apply but the support and unloading comes instead from temporary heel wedges that can be placed inside the shoe. Please move on to ‘The Perfect Shoe’ for now and see the information on heel wedges in the ‘Reducing Irritation chapter’.
Plantar Fasciitis:
The following strapping technique can help reduce stress and strain that would ordinarily run through the plantar fascia during standing and walking.
In order to strap your foot correctly, you should opt for rigid sports tape instead of materials that stretch, like rock tape or K-tape. Your local pharmacy should stock rigid sports tape, approximately 4 cm wide.
It is helpful to have a household member apply the tape as per the video, however it can be applied alone. Some patients have said that placing the affected foot (forefoot) on a chair while standing is an easy way to apply it. Others prefer to be seated. Keep strapping your foot until the pain has gone and be careful that your skin doesn’t react badly to the glue on the tape. If itchy or sore please remove and wash your feet and follow instructions above.
*Please note that low dye strapping is less crucial for the other conditions.
Selecting the appropriate footwear is crucial for supporting the healing process of foot conditions like Plantar Fasciitis and Achilles Tendonitis.
It’s essential to distinguish between cushioning, which is less important, and control, which is vital.
Focus on evaluating the shoe’s OUTSOLE/MIDSOLE for its structural integrity, rather than being swayed by the soft liner and arch support.
The resistance test, as shown in the accompanying video, is a practical way to assess this.
Support, rather than cushioning, is what your heel and arch require. As demonstrated, your shoes should resist bending when you apply force, indicating the necessary rigidity. Avoid flat, flexible footwear, walking barefoot, or wearing slippers and flip-flops, even indoors. Consider using heel wedges in flat shoes to elevate the heel by about 6 – 10mm, with further details available in the subsequent chapter.
A well-made walking or running shoe from a reputable brand, such as Asics, is advisable. However, not all models provide the needed sole firmness, so testing the shoe physically in-store is key.
Given the yearly changes in sports shoe features, recommending a specific model is challenging. Look for the qualities mentioned and seek advice from a footwear specialist to find the most suitable option. Currently, the Asics Gel 2000 SX, known for its wider fit, and other models like Brooks Adrenaline and New Balance walkers (624 or MX857V3), excluding any with Fresh Foam technology, are recommended for their firmness. Nike’s Air Max or Air Force also offer rigid soles.
An ideal sports shoe features a heel to toe drop of around 15mm, crucial for foot health. If sports shoes are impractical for daily wear, consider wearing them during commutes and switching to work-appropriate footwear on arrival at work.
Note that sports shoes designed for cushioning lack the necessary sole firmness and should be avoided.
For stylish yet supportive street, casual, or office shoes, Dr Karl recommends Bared Footwear, which incorporates a steel shank in the sole for enhanced support and durability.
Visit www.bared.com.au for options. Australian patients can enjoy a 10% discount with Dr Karl’s referral code SHP10, along with complimentary shipping and returns. They also offer remote fittings and sizing.
Firm hiking / trekking shoes and boots are also great to wear during your recovery. Merrell / Salomon / North Face.
Safety boots: Ascent and surprisingly – Skechers! They made a firm soled boot with a safety cap.
With all heel and arch pain conditions, you should attempt to reduce any deep tissue inflammation (usually not visible to the naked eye but sometimes visible in acute Achilles Tendonitis) via the use of cold compress or ice packs. This is not for pain relief but to accelerate healing.
Plantar Fasciitis and arch pain
Plantar Fasciitis usually involves irritation at the attachment on the heel or through the arch of the foot. It is assumed that the start-up pain is due to inflammatory change that develops in the foot during periods of sleep or rest and to this end, the application of a cold compress / ice pack reduces this internal reaction, which is designed to protect the area but slows down healing.
You should apply an ice pack with a horizontal leg position, and gentle pressure against the painful part of your foot on a daily basis – 10 minutes on and 10 minutes off – and repeat at least 3 times before bed. You may apply throughout the day if your schedule permits. Keep an eye on your skin to avoid freezer burn and seek the advice of your doctor if you are diabetic.
Dr Karl does not suggest heat packs for any condition.
Achilles Tendonitis, Tendinosis or Bursitis
Rest your heel and Achilles tendon on an ice pack, placed on a table or footstool on a regular basis as above. If you feel no change or long term benefit from ice packs after one week of daily application then you can stop.
Patients with an Achilles tendon condition (and Peroneal / Tibialis tendon condition) should insert heel wedges inside the back of both shoes in order to elevate the heel. (Always insert inside both shoes to avoid lower back and hip irritation). These are to be used on a temporary basis and should be removed once the condition has resolved. These heel lifts/raises/wedges can be purchased online. They commonly come in a red colour and you should look for a pair of 9 or 10mm lifts (height at the back edge of the wedge) that will offer approximately 6mm of elevation in the centre of the device. Mediums are slimmer in width and Large are wider.
Using a search engine, please type words such as Red, EVA, heel lifts, heel wedges, heel raisers, 9mm, 10mm. We are not affiliated with any suppliers but here is what they look like.

Strategies for Prevention and Recurrence
Managing expectations for the healing process of these conditions is crucial, as they seldom resolve overnight. However, you can anticipate gradual improvement in the days and weeks ahead. The recovery timeline varies significantly, ranging from 1 to 8 weeks, influenced by factors such as the severity of your condition, daily activity level, lifestyle, occupation, body weight, and the duration for which you’ve experienced the issue.
A key indicator of progress is a noticeable decrease in pain throughout the day, particularly the reduction of discomfort during your first steps each morning. This alleviation of morning pain is a positive sign of healing.
To effectively monitor your recovery, record your pain levels at various times throughout the day on a scale from one to ten. Observing a consistent decrease in morning pain and a quicker subsidence of discomfort are encouraging signs that your condition is healing. This methodical approach to tracking your pain can provide valuable insights into your recovery process and help you gauge the effectiveness of your treatment strategy.
After successfully treating heel pain conditions such as plantar fasciitis or Achilles Tendonitis taking preventive measures can help avoid a relapse. This includes continuing to wear appropriate footwear that provides proper support, reducing excessive strain on the feet.
Regularly incorporating calf muscle stretches into your routine can significantly alleviate long-term heel strain. Proactively managing risk factors such as obesity, overuse, and the choice of worn or inappropriate footwear is crucial in preventing the recurrence of foot conditions.
Listening to your body and respecting its limits is essential; ignoring pain or warning signs can lead to the return of foot issues.
Key preventive strategies include:
- Ensuring a good range of motion in the calves.
- Avoiding flat and flexible shoes as your primary footwear—use them sparingly and rotate your shoes regularly.
- Opting for functional shoes that provide support and rigidity for exercise or prolonged walking.
- Stretching your calf muscles at the day’s end, particularly after physical activity.
- Being vigilant for early heel pain indicators, such as tightness in the heel or arch or the sensation of a pebble in your shoe.
- Watching out for signs of calf tightness or cramping.
- Avoiding walking barefoot or in flip-flops for long periods.
- Exercising caution with calf-raising exercises and activities that place excessive load on the forefoot.
- By prioritising these preventive measures and making informed lifestyle choices, you can significantly reduce the risk of foot conditions reoccurring and maintain healthy feet.
It’s important to remember that tight calf muscles, often exacerbated by the frequent use of soft-soled shoes, flip-flops, or thongs, are a common cause of these conditions. Regularly inspect your footwear for wear and tear and maintain an adequate range of motion in your calves.
If you’re uncertain about your foot conditions diagnosis or have concerns about the appropriate treatment, consult your doctor about getting a referral for an ultrasound, which can provide a definitive diagnosis.
If your condition happens to become chronic and there is residual pain you must continue with the treatment plan above but consider adding:
- Shock wave therapy ( All conditions)
- Cortisone injection guided with ultrasound (Plantar Fasciitis and retrocalcaneal bursitis, not Achilles Tendonitis)
- Custom orthotics, designed by a podiatrist, with gentle arches that just touch and hold the sole of your foot, without pushing. These should be made from a slimline, firm material that doesn’t compress under body weight. ( Plantar Fasciitis )
If your Plantar Fasciitis or Achilles Tendonitis / tendinosis happens to become chronic and acute, leading to very high pain levels and frequent limping you must continue with the treatment plan above and consider the use of an immobilisation boot. You will need a full height boot which stops just below the knee and avoids the shorter versions that just cover the ankle. Dr Karl’s favourite brand is the Ossur rebound air walker.
You should take it off to sleep, shower and drive but wear it whenever you are standing or walking. Use it until the pain levels drop significantly and continue with the At Home Treatment Plan.
The above treatments are not always needed but if your condition is a slow healing condition they can accelerate the healing process, as long as the foundations of the treatment plan are in place.
When searching for the ideal podiatrist to treat foot conditions like plantar fasciitis and achilles tendonitis, it’s crucial to find a sports podiatrist who routinely conducts biomechanical assessments.
It’s important to enquire about their success in treating these specific conditions. Opting for a specialised sports podiatrist is preferable to a general podiatrist who may spend a significant portion of their time on tasks like cutting toenails or shaving corns and callus from the skin.
A sports podiatrist can provide treatments such as custom orthotics or a moon boot, but they may provide advice that differs to the advice provided here. To this end, you may wish to politely refuse the treatment plan that may be suggested by other practitioners.
If you’re interested in booking an appointment with Dr Karl Lockett, you can do so using our online booking system here.
Dr Karl also offers zoom consultations or telehealth.